THE EXCHANGE | Newsletter June 2020
Published on: Jun 30, 2020
Medanta Sets up a Dedicated COVID Hospital
Collaborates with other hospitals and corporates to operationalize Medeor in
Manesar, Haryana
Responding to the unprecedented and rapidly evolving public health challenge, Medanta in partnership with Fortis, Artemis and Medeor Hospitals recently set up a dedicated COVID hospital, first-of-its-kind in Gurugram. Medeor in Manesar will work as an independent clinical unit for the treatment of mild, moderate and severe cases of COVID-19. The hospital will follow all standard protocols and guidelines laid down by the Indian Council of Medical Research (ICMR). The hospital addresses all infrastructure pre-requisites for a COVID-19 hospital - ICUs, ventilators, negative pressure isolation rooms, testing, re-testing, surveillance facility.
A team of Medanta doctors and nurses has been deployed at Medeor along with staff from other hospitals. Medanta was instrumental in setting up the facility, providing equipment, establishing infection control and treatment protocols, and training staff.
In addition to setting up the hospital, Medanta has also been instrumental in setting up ‘Gurugram COVID-19 Volunteers Group’ with other hospitals and corporate organizations to support the local administration fight the epidemic in the state. The group is focused on ramping up testing of COVID-19, improving capacity of isolation wards, hospital and intensive care unit beds, securing ventilators and personal protective equipment, and training health workers.
Dr Naresh Trehan
Chairman and Managing Director, Medanta
“The dynamic and rapidly evolving situation demands us to think laterally and operate cross functionally. We collaborated with the government, corporates and other private hospitals to ramp up the state’s capability to fight the pandemic. We will continue to engage with all stakeholders to address this challenge collectively.”

Dental Implants for Terminal Dentition
Nutrition is one of the important pillars of good health and the oral cavity is the gateway for it. Sometimes, the absence of many teeth or the presence of unrestorable teeth leads to a condition called Terminal Dentition which results not only in poor oral health but also attributes to several other disorders such as:
• Diabetes
• Stomach problems
• Jaw joint pains
• Forgetfulness
The treatment for Terminal Dentition involves the removal of all bad teeth and replacement with new implant-supported fixed dentition. The Dental Surgery department at
Medanta - Gurugram has the expertise and technology to address the most complex cases of terminal dentition. The team, trained from AIIMS, has successfully done over 8,000 implants and has unparalleled width and depth of experience in full mouth rehabilitation.
The treatment starts with a thorough evaluation of the patient and radiographic assessment with the help of Dental Cone Beam CT (CBCT) followed by a comprehensive assessment and a customized treatment plan. In the procedure, the surgeon removes all the bad teeth and places dental implants at the same time. Temporary teeth are fixed within the following 2-3 days. Over the next three to five months, the implants fuse with the bone and after that, the temporary teeth are replaced by a new set of permanent teeth. Thus, the patient receives a set of new well-functioning teeth in a short span of time which not only improves their quality of life but also boosts their self-confidence.
All-on-four Treatment
This concept was developed to maximize the use of available remnant bone in atrophic jaws, allowing immediate function and avoiding bone-grafting procedure thus reducing the treatment cost and patient morbidity. The protocol uses four implants in the anterior part of complete edentulous jaws to support a provisional, fixed and immediately loaded prosthesis. The two most anterior implants are placed axially, whereas the two posterior implants are placed distally which are angled to minimize the cantilever length. This allows the application of prostheses with up to 12 teeth, thereby enhancing masticatory efficiency.

Case Study
A 65-year-old female with no major comorbidities reported to Medanta - Gurugram with a failing bridge. Following a thorough clinical examination, 3D scan (CBCT) was done and the patient was evaluated for possible treatment options. The remaining bone was much less and bone grafting was not intended. All-on-four treatment plan was proposed wherein all the teeth can be supported with the help of only four implants. The proposed approach involves a painless, minimally invasive surgery with quick, predictable results within a day.
The patient was tested for all comorbidities and scheduled for the surgery. During an hour-long procedure, under local anesthesia, all the infected and bad teeth were removed and implants were placed at the same time. Temporary teeth were fixed the next day and the patient resumed a normal diet. The patient was later discharged with oral hygiene instructions and kept on regular follow up. After three months, as the healing progressed, temporary teeth were replaced with permanent teeth. The patient was asked to maintain oral hygiene and advised half-yearly follow up.
Dental procedures require a close contact between the dentist and patient’s oral cavity, putting each at higher risk of contracting the COVID-19 infection. Medanta Institute of Dental Sciences is offering the full spectrum of dental treatments in the safest possible environment. We have ensured strict adherence with international safety guidelines for dental clinics for a COVID-Safe experience.
medanta.org/dr-ankur-rustagi/
medanta.org/dr-satyavrat-arya/
medanta.org/dr-amrita-gogia/
Medanta’s Experience Promising Clinical Outcome in Medically
Inoperable Stage I Lung Cancer with Radiosurgery
Lobectomy with sampling or dissection of mediastinal lymph nodes is considered to be the standard therapy for operable, clinical stage I, non-small-cell lung cancer (NSCLC). This has been challenged with the advent of Stereotactic Ablative Body Radiotherapy (SABR); also called Stereotactic Body Radio-Therapy (SBRT), and has resulted in local control of more than 90% cases of tumours with medically inoperable and operable clinical stage I NSCLC. Overall survival after SABR is better than conventional radiation. SABR delivers ablative doses of radiation to tumours in one to six fractions. 250-360 radiation fields are delivered from various angles to converge on a target, so that the dose is sharply reduced within a few millimetres beyond the target, sparing nearby lung, heart, oesophagus and spinal cord from radiation-induced damage. SABR is the recommended treatment for medically inoperable, node negative stage I-II NSCLC. Findings from population-based studies using propensity-matched analyses, phase II prospective studies and pooled analysis of phase III studies (STARS and ROSEL) have shown that SABR is associated with overall survival similar to that of surgery in patients even with operable stage I NSCLC and could be an option for treating operable stage I NSCLC.
Lung cancer is a disease that affects patient of sixth decade and beyond, and there is strong co-relation of smoking with lung cancer. Such patients have pre-existing cardiac co-morbidity as well as emphysema or bronchiectasis that precludes major lung resection like pneumonectomy or lobectomy due to poor cardio-pulmonary reserves.
 Cyberknife
Cyberknife
The advantage of SBRT is its feasibility for patients with numerous comorbidities, high anaesthesia risk or medically inoperable condition. Good tolerance of SBRT has been reported even for octogenarians and patients with severe chronic obstructive pulmonary disease (III–IV COPD). There can be different platforms for delivering SABR using either Cyberknife Radiosurgery or high-end linear accelerators with gating methodology. Recent advent of Proton Therapy although tested at the MD Anderson Cancer Centre mandates making the lung stationary and gating systems are not yet very robust to pervert proton beam from overshooting the target due to constant lung motion. One prerequisite for delivery of SABR is the ability to compensate for lung motion during treatment, which can be accomplished with techniques like tumour tracking (Cyberknife), gating and breath hold (Linear Accelerator). Some centres have used fiducial placement in lungs. However, with COPD, there is a very high risk of pneumothorax that can jeopardize the treatment and worsen patient’s overall condition.
Case Study
Long-term outcomes of SABR in a case of cT1N0M0 NSCLC who was not a candidate for surgery due to multiple comorbidities
67-year-old male, reformed heavy smoker with 20 years of diabetes history, on insulin presented at Medanta - Gurugram in 2014. He had a history of coronary artery disease (CAD) for which he underwent angioplasty (PTCA). He was also diagnosed with dilated cardiomyopathy with ejection fraction of 25%. He had longstanding history of COPD with gradual worsening of pulmonary function, FEV1 at 35% of the predicted value (GOLD III). His blood chemistry parameters were acceptable except raised blood urea/creatinine (66mg/dl/2.2mg/dl) due to diabetic nephropathy. During one of the episodes of COPD exacerbation, pulmonologist performed HRCT thorax which showed a well-defined solid nodule (2.5cm x 2cm) in the superior segment of right lower lobe. Non-contrast PET CT scan was performed. The solid nodule showed heterogenous contrast enhancement with intense FDG uptake (SUV Max: 15.5). There was no distant metastasis or mediastinal/hilar lymphadenopathy.
To confirm malignancy, patient was referred to Interventional Radiology for tissue sampling for the nodule. He was informed about the options of trucut biopsy versus fine needle aspiration cytology (FNAC) with pros/cons of each procedure including high risk consent for pneumothorax. He opted for needle cytology. FNAC was uneventful and Cytopathology report confirmed the diagnosis of malignancy (squamous cell carcinoma). Case was discussed in Medanta’s cross-functional Tumor Board and in view of comorbidities (Charlson Comorbidity score 2-COPD, CAD/ PTCA, diabetic nephropathy), it was decided to offer SABR with curative intent.
Patient was explained about the process of SABR, including different modalities of delivery. He was planned on Cyberknife Radiosurgery system using tumor tracking technique (X-sight lung tracking with respiratory synchrony system) without fiducial placement. Since he had poor lung reserves, he was not a candidate for SABR using breath-hold technique. In Cyberknife planning, one mm section CT scans were acquired in end inspiratory, end expiratory phases as well as free breathing to map the trajectory of the lung motion and the tumour motion
within the lung. Simulation on patient was done as per protocol and tumor was visible on both the Cyberknife cameras (2- View) for real time tumour tracking. Tumor and normal tissues were delineated on CT scan for planning. Ablative dose of 60 Gy in 3 fractions was planned to be delivered on three consecutive days. Software based planning was done on Multiplan system and best plan was chosen based on the target and normal tissue dose parameters. Patient completed the planned treatment in three days uneventfully.
First follow up post-treatment was done at three months to assess the response and an HRCT scan showed minimal soft tissue residue with necrosis. PETCT performed at six months showed complete disappearance of FDG avid disease and was replaced by post-treatment fibrosis in the treated area. Post-treatment pulmonary function test showed no deterioration of lung function parameters. Patient has completed six years of follow-up with no signs of disease recurrence or metastasis and is being managed for comorbidities.
SABR/SBRT offers patients with inoperable Stage I
NSCLC the advantages of a high local control /cure rate and low treatment-related mortality. Opting for either no treatment or conventional radiotherapy alone would lead to poor survival and compromised quality of life. Therefore, SBRT may be a better treatment option than resection especially in cases with significant comorbidities.
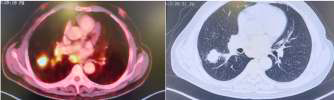 Pre SABR
Pre SABR
 Post SABR @ 6 months
Post SABR @ 6 months
medanta.org/dr-shyam-singh-bisht/
medanta.org/dr-tejinder-kataria/
COVID-19 Home Isolation
15-days Remote Home care Package
Rs. 4 ,900
COVID CARE
- Vitals monitoring tool with built-in critical alert mechanism
- Daily remote Monitoring by trained nurse
• 4 Doctor Consultations
• 1 Dietician consultation
Rs. 9 ,900
ADVANCE COVID CARE
- Vitals monitoring tool with built-in critical alert mechanism
- Daily remote Monitoring by trained nurse
- 4 Doctor consultations
- 1 Dietician consultation
- N-95 masks, 3 ply mask, Gloves, Sanitizer, SPO2 meter, Digital Thermometer
Rs. 11 ,900
ADVANCE PLUS COVID CARE
- Vitals monitoring tool with built-in critical alert mechanism
- Daily remote Monitoring by trained nurse
- 4 Doctor Consultations
- 1 Dietician consultation
- N-95 masks, 3 ply mask, Gloves, Sanitizer, SPO2 meter, Digital Thermometer, BP machine
Rs. 21 ,900
COMPLETE COVID CARE
- Vitals monitoring tool with built-in critical alert mechanism
- Daily remote Monitoring by trained nurse
- 4 Doctor consultations
- 1 Dietician consultation
- COVID test
- *PPE kit
- N-95 masks, 3 ply mask, Gloves, Sanitizer, SPO2 meter, Digital Thermometer, BP machine
Quantities as included in the packages:
N-95 masks - 4
3 ply masks - 17
Gloves - 100
Sanitizer - 2
PPE kit - 4
Patient can avail following additional services
Psychologist Consultation*
Home delivery of medicines*
*Chargeable on actuals
As per government guideline, confirmed mild cases of COVID-19 may not require hospital stay if they have the requisite facility of self-isolation at home.
For Enquiry, call: +91 124 4834 566






